One Practice for TRD, Perinatal, and Adolescent Psychiatry
Three populations rarely share one outpatient psychiatry practice: the patient already two antidepressants in who needs TMS or Spravato, the mother adjusting medications across pregnancy, and the parent vetting providers for a twelve-year-old. This brief proposes the seventeen surfaces a single practice needs to serve all three credibly. Built for the Dallas outpatient psychiatry practice that wants to be the regional destination for treatment-resistant depression rather than another general medication-management clinic.
See It Move
This is the brief, rendered as a working product rather than a deck. Every surface below is a real page in it. There is no single-page router and no route illusion: the practice is twenty-five separate HTML pages, each one its own URL, because a medical practice's insurance page and crisis page have to be linkable, printable, and findable on their own. The motion is earned rather than decorative. The trajectory chart draws, the outcome counters count, and the first-visit timeline advances when each one scrolls into view, and every one of them is frozen for a visitor whose system asks for reduced motion.
The video plays inline at the same visual size as the section screenshots so the buyer reading the brief can see the architecture in motion before they read the architecture in language. A still psychiatry-practice site can describe the journey from a 9pm search to a same-week evaluation. A psychiatry-practice site that the buyer can watch behave on their own laptop demonstrates the journey instead.
The Founder Signs a Treatment Commitment

The single most important surface a psychiatry website can carry is also the one most psychiatry websites omit entirely. The founding physician's voice, in the first person, signed at the foot. A patient who has tried two antidepressants without relief is not in the market for a brand voice paragraph that opens with "we believe mental health care should be personalized." She is in the market for a person, with a name and a face and a residency, willing to put a sentence in writing about what the work will look like if she walks in.
The brief proposes the credentials of a board-certified psychiatrist with twenty-two years in practice be rendered as a signed letter, in the founder's voice, on the second surface of the home page, where every researching patient and every referring primary-care physician will see them before they see anything else. The residency, the teaching credential, the leadership history. Those facts are the credential. The signed letter is the surface that makes them visible.
The structural commitment in the third paragraph is the line that closes the patient. "I am the one who will tell you when a medication adjustment is the right next step, when TMS is the right next step, when Spravato is the right next step, and when the right next step is to keep doing what you are doing because it is finally beginning to work." That sentence does the work the entire rest of the page rests on. It says the practice is willing to recommend doing nothing. A psychiatry practice that will tell a patient her current regimen is working and to stay the course, when the practice could have billed her for a new evaluation, is a practice that has earned the patient's trust before the first appointment.
Services Indexed by Patient Search Behavior
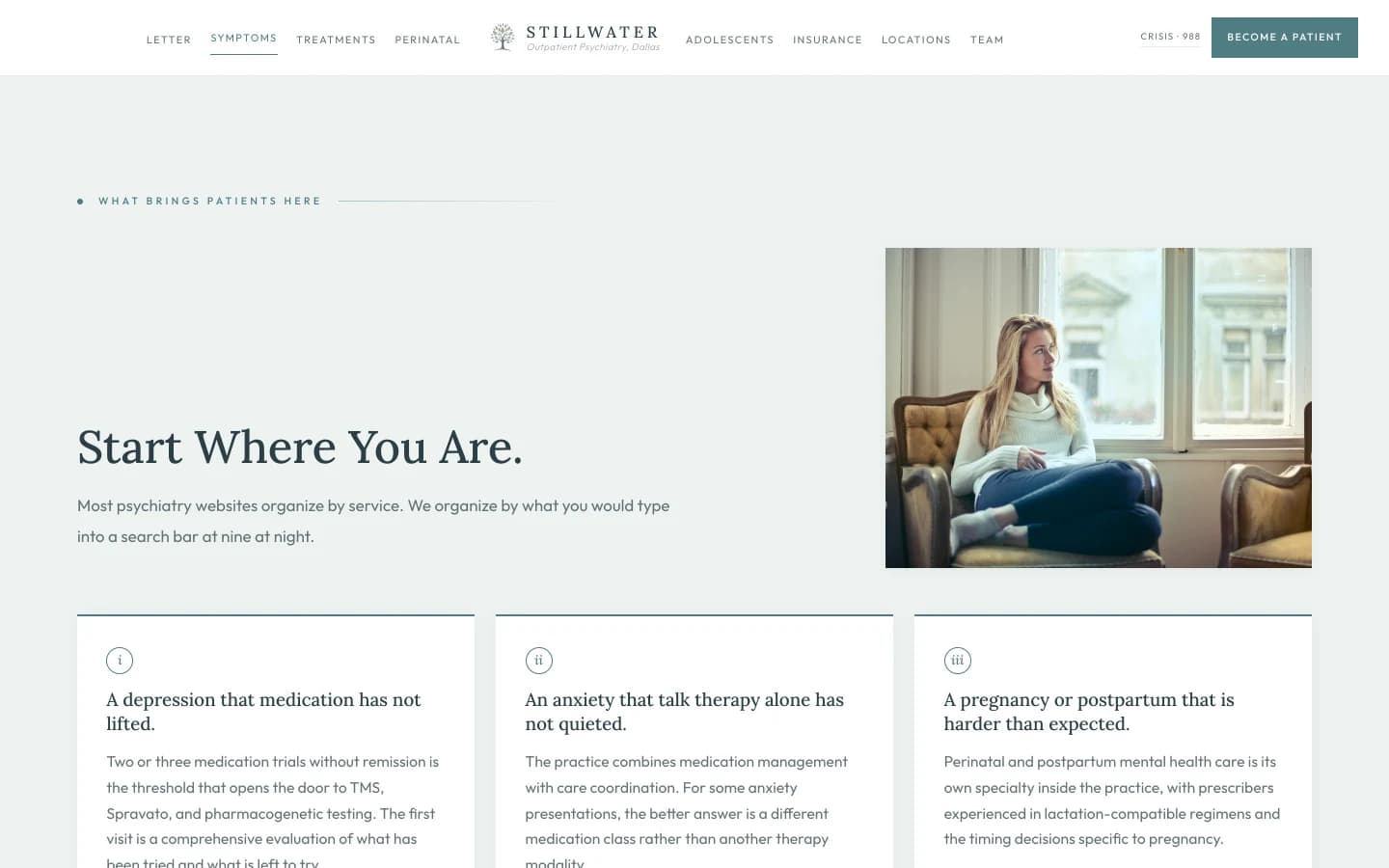
The standard outpatient psychiatry website opens its services section with the phrase "Our Services" and lists Psychiatry, Medication Management, Therapy, TMS, Spravato, in alphabetical order. That ordering is convenient for the practice and useless for the patient. A patient does not arrive at the page knowing she needs Spravato. She arrives knowing the antidepressant her primary care doctor put her on six months ago has stopped working, and her sister sent her a link, and she has thirty seconds before she closes the laptop again.
So the brief reorganizes the entry surface around what the patient is actually searching for. Six symptom-shaped doorways, each one written in the patient's voice rather than the practice's. "A depression that medication has not lifted" is the doorway to the TRD architecture below. "A pregnancy or postpartum that is harder than expected" is the doorway to the perinatal surface. "A teenager who is not okay" is the doorway to the adolescent surface. "A medication regimen that needs a second opinion" is the doorway to GeneSight and chart review. Each doorway leads to the right destination inside the practice without forcing the patient to learn the practice's vocabulary first.
The supporting paragraph above the grid is the structural admission that earns the section. "Most psychiatry websites organize by service. We organize by what you would type into a search bar at nine at night." That sentence does two things at once. It tells the patient the practice has thought about her experience of finding it. And it tells the referring primary-care physician, the OB, the pediatrician, that the practice has built its intake around how patients actually present. A practice that admits the search-bar reality has done more work on its front door than ninety percent of its competitors.
The PHQ-9 Lives on the Page
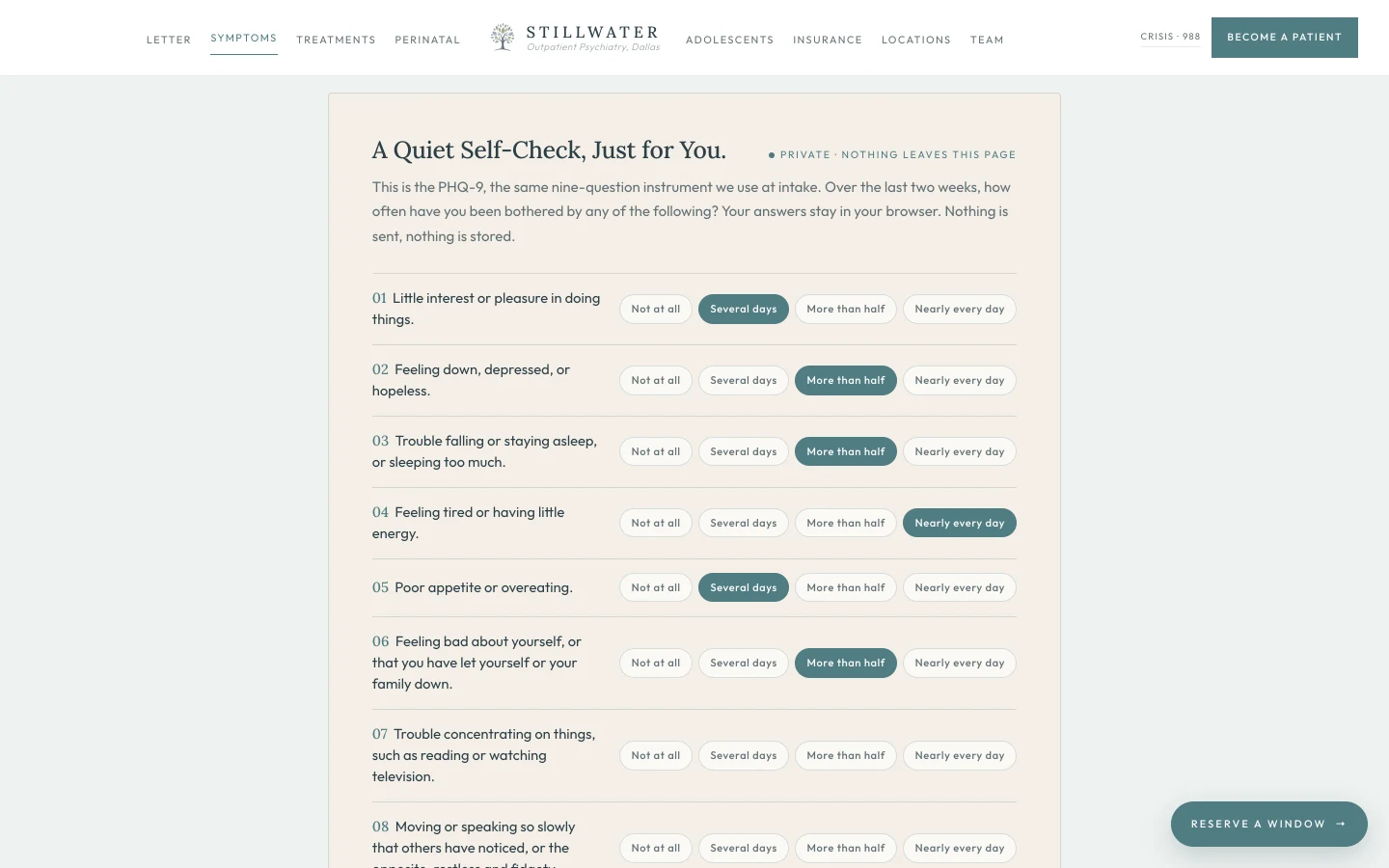
The PHQ-9 is the most clinically literate move on the entire homepage, and almost no outpatient psychiatry site in the country renders it inline. Patients who arrive at the practice's door already know the instrument, because their primary-care office handed them a paper copy six months ago and asked them to fill it out in the waiting room. Letting the patient take it again, here, in private, with no submission and no telemetry, is the editorial move that says the practice understands what it is asking for when it asks the patient to walk in.
The five-tier scoring band is the architectural commitment that follows. A score of zero through four returns a quiet headline that says reflective, not symptomatic, with a paragraph that names the PHQ-9 as one window and offers the door if the patient wants it. A score of ten through fourteen returns "this is exactly what we treat," with a same-week evaluation offer. A score of twenty or above returns "please call us today," with both phone numbers in the body and a 988 line for crisis. A positive answer to question nine, regardless of the total score, automatically appends a soft-amber 988 safety note that names calling as a conversation rather than a commitment. The scoring logic was built around the way the practice would actually triage the score on a paper copy. The patient gets the same triage in their browser, in private, before any call is placed.
The clinical literacy of this single component is the load-bearing reason a patient who has tried two SSRIs without remission keeps reading instead of closing the tab. The brief proposes that this surface alone earns more new-patient calls than any paid search campaign the practice could fund.
When the Last Antidepressant Didn't Work
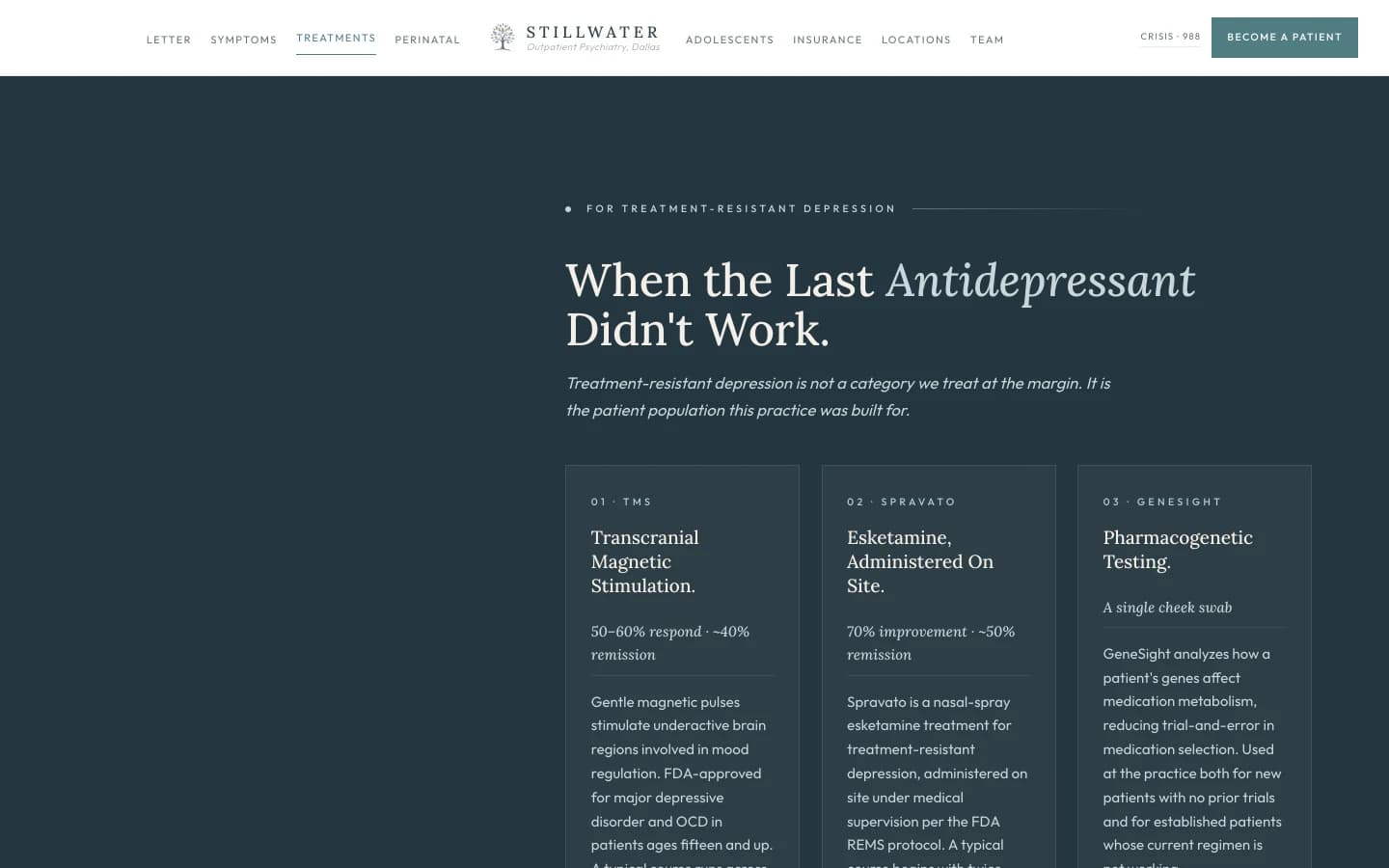
This surface is the spine of the entire brief, and it is the surface most outpatient psychiatry practices in Dallas cannot render at all. A general medication-management practice that does not offer TMS and Spravato has no card to write here. It can only describe medication adjustment and refer the patient elsewhere when the medications stop working. The practice the brief envisions carries all three of the standard treatment-resistant-depression interventions on site, which means this surface is the single largest competitive moat the practice has, and the page should render it accordingly.
The three cards are deliberately written with the actual outcome percentages the FDA has approved for the treatments. TMS at fifty to sixty percent response and approximately forty percent remission. Spravato at seventy percent improvement and approximately fifty percent remission. Those numbers are not aspirational; they are the trial data the manufacturers cite and the FDA approvals reflect. Publishing them in the same typography as the headline rather than burying them three clicks deep under a "Learn More" button is the structural commitment that earns the patient's trust. A patient who has tried two SSRIs without remission reads "fifty percent remission with Spravato" and understands, for the first time in some cases, that there is a real probability she has not yet exhausted the options.
The footer line at the bottom of the surface does the operational work. "All three offered on site. Medical District for TMS and Spravato. Both locations for medication management and GeneSight." That sentence pre-empts the patient's next question, which is always logistical. Where is this delivered. How often. Do I have to drive to a hospital. The answer is no, the entire treatment ladder for treatment-resistant depression is available at a Medical District address, with the medication management arm available at a Park Cities address, and the patient can begin where she lives.
Plotting the PHQ-9 Over Time
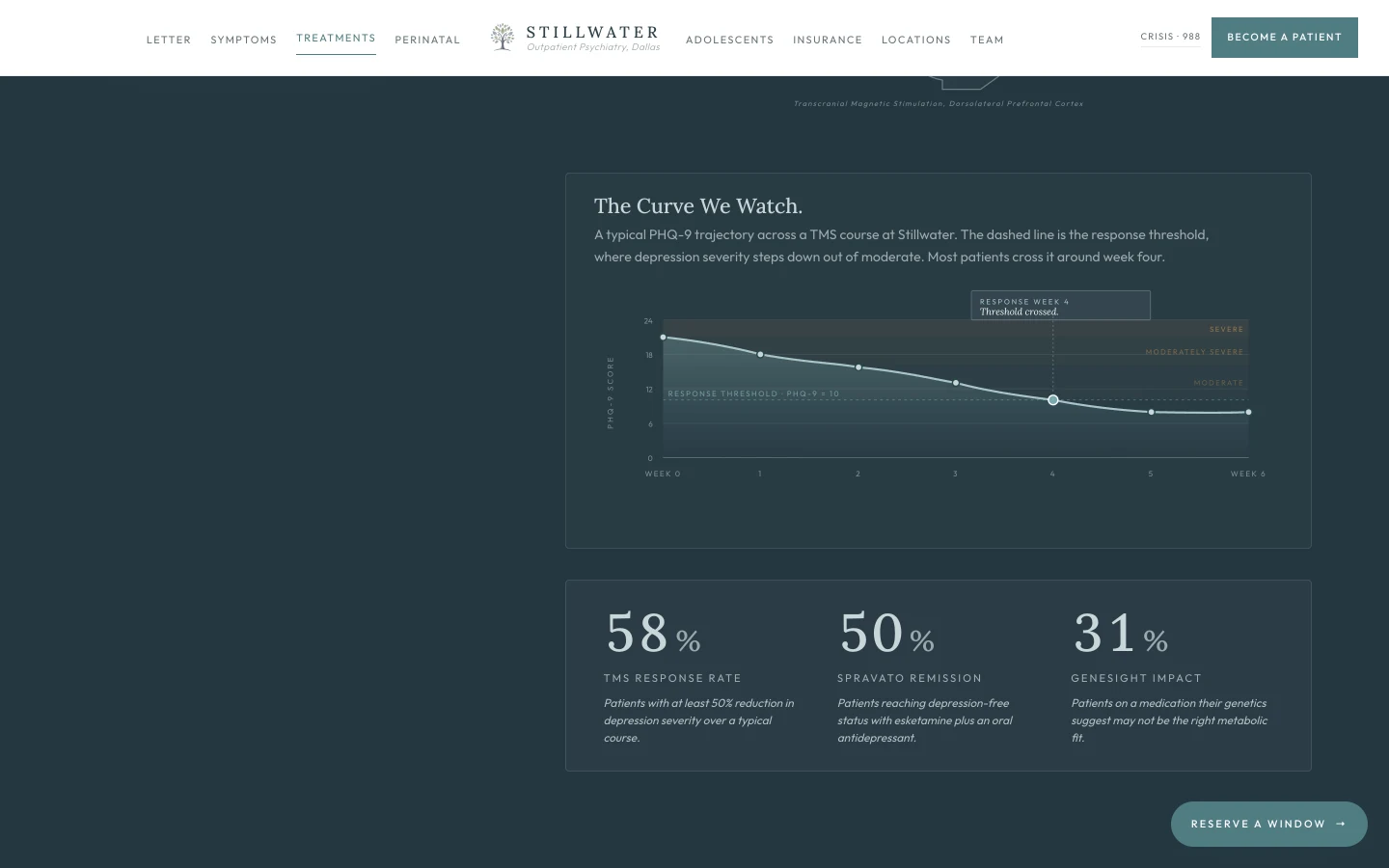
The cards above this surface name the percentages that make TMS, Spravato, and GeneSight worth offering. This surface renders the percentages as a journey rather than a statistic. A PHQ-9 score of twenty-one at week zero is a patient who could not get out of bed last Tuesday. A PHQ-9 score of ten at week four is the same patient who has gone to her sister's house for dinner once and made it through. The chart names that arc in the patient's vocabulary, not the practice's.
Most psychiatry sites that quote TMS efficacy quote it as a static fifty to sixty percent number on a brochure card and trust the patient to imagine the trajectory. The brief proposes drawing the trajectory instead, with the response threshold visible as the dashed teal line, the four-week crossing visible as a labeled annotation, and the three counters at the bottom animated to count up the moment the route becomes visible. A patient who has tried two SSRIs without remission reads "around week four, most patients cross the threshold" and understands, for the first time in some cases, that the wait between starting a treatment and feeling like herself is measurable, finite, and short relative to the years she has spent without remission.
The animation does the editorial work the static chart cannot. The line draws from week zero to week six in a 2.2-second stroke-dashoffset reveal. The data dots pop in sequentially with a cubic-bezier overshoot stagger. The annotation card fades in last. The three counters tick from zero to their target values with cubic easing. Every visit re-runs the sequence, because every visit is a different patient who needs to see the curve drawn in front of her own eyes.
Pregnancy Is Not a Reason to Stop Treatment

Perinatal mental health is the specialty most outpatient psychiatry sites either omit or list as a one-line bullet under "Services." The brief proposes promoting it from a service item to a destination surface, because perinatal psychiatry is one of the highest-trust, highest-search-volume, lowest-supply specialties in the entire field, and a practice that pairs a board-certified psychiatrist with a perinatally-experienced PMHNP can credibly own the category in DFW.
The credential is the PMHNP's clinical history. Years in maternal and infant care at a Dallas hospital, then transition into psychiatric practice. That trajectory is what perinatal mental health requires. A nurse practitioner who has been in a maternity ward, who has watched a postpartum patient with untreated bipolar disorder unravel in a unit, who knows what a lactation-compatible SSRI dose actually looks like at four weeks and at twelve weeks. The brief renders that history as the structural argument for the surface. The patient does not need to be told the practice cares about pregnancy. She needs to be told the person treating her has held a postpartum mother in a unit and knows, by name, the medications that finished the night safely and the ones that did not.
The third paragraph is the operational commitment that distinguishes the practice from the cautious-by-default behavior that most non-specialist providers fall into during pregnancy. "We adjust regimens with the OB in the loop. We are honest about the trade-offs and we put them in writing so the patient can make the decision rather than have it made for her by the most cautious provider on the team." That sentence is the architectural rebuttal to the failure mode the patient is most afraid of. Most pregnant patients with active mental illness are told to discontinue medication on the day of the positive test, by a provider who has not read the most recent literature on the specific molecule in question and who is defaulting to abstinence as the conservative position. A practice that is willing to keep treating, with the OB informed and the patient informed and the trade-offs in writing, is the practice that earns the referral from the OB who is tired of patients relapsing in the second trimester because they were taken off lithium without a plan.
Adolescent Psychiatry From Age Twelve
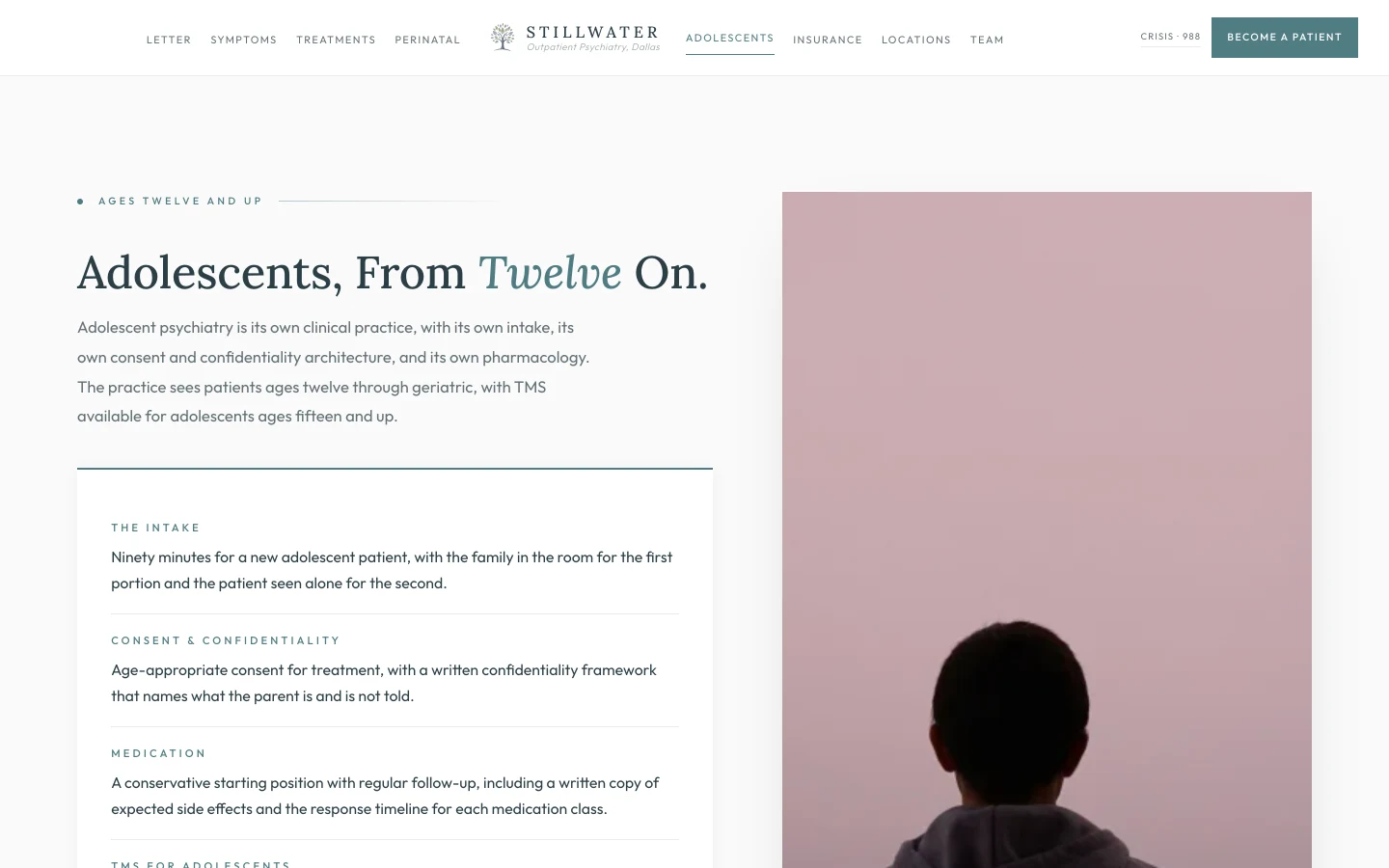
The adolescent surface is the one most outpatient psychiatry sites get wrong by treating a fourteen-year-old as a smaller version of an adult. Adolescent psychiatry is not adult psychiatry at a lower dose. It is its own intake architecture, its own confidentiality framework, its own pharmacology, and its own family-system clinical reality. The brief proposes a surface that renders the adolescent intake as the distinct practice it actually is, with four operational lines a parent can read and recognize.
The intake line is the first thing a parent of a depressed teenager wants to know. "Ninety minutes for a new adolescent patient, with the family in the room for the first portion and the patient seen alone for the second." That sentence answers the question every anxious parent has when they call. How long. Who is in the room. When am I asked to step out. A practice that names that architecture on the page rather than making the parent ask is a practice that has thought about the parent's experience.
The TMS line is the credentialed differentiator that most general psychiatry practices in DFW cannot match. "FDA-approved at age fifteen and above for major depressive disorder, delivered at the Medical District location across weekday sessions over several weeks." A fifteen-year-old in a Highland Park or Lakewood high school whose depression has not responded to two SSRIs has an FDA-approved option that almost no other outpatient practice in the region can offer on site. The brief makes that fact visible to the parent who is currently considering driving to Houston or Austin. They do not have to.
If Your Teenager Is
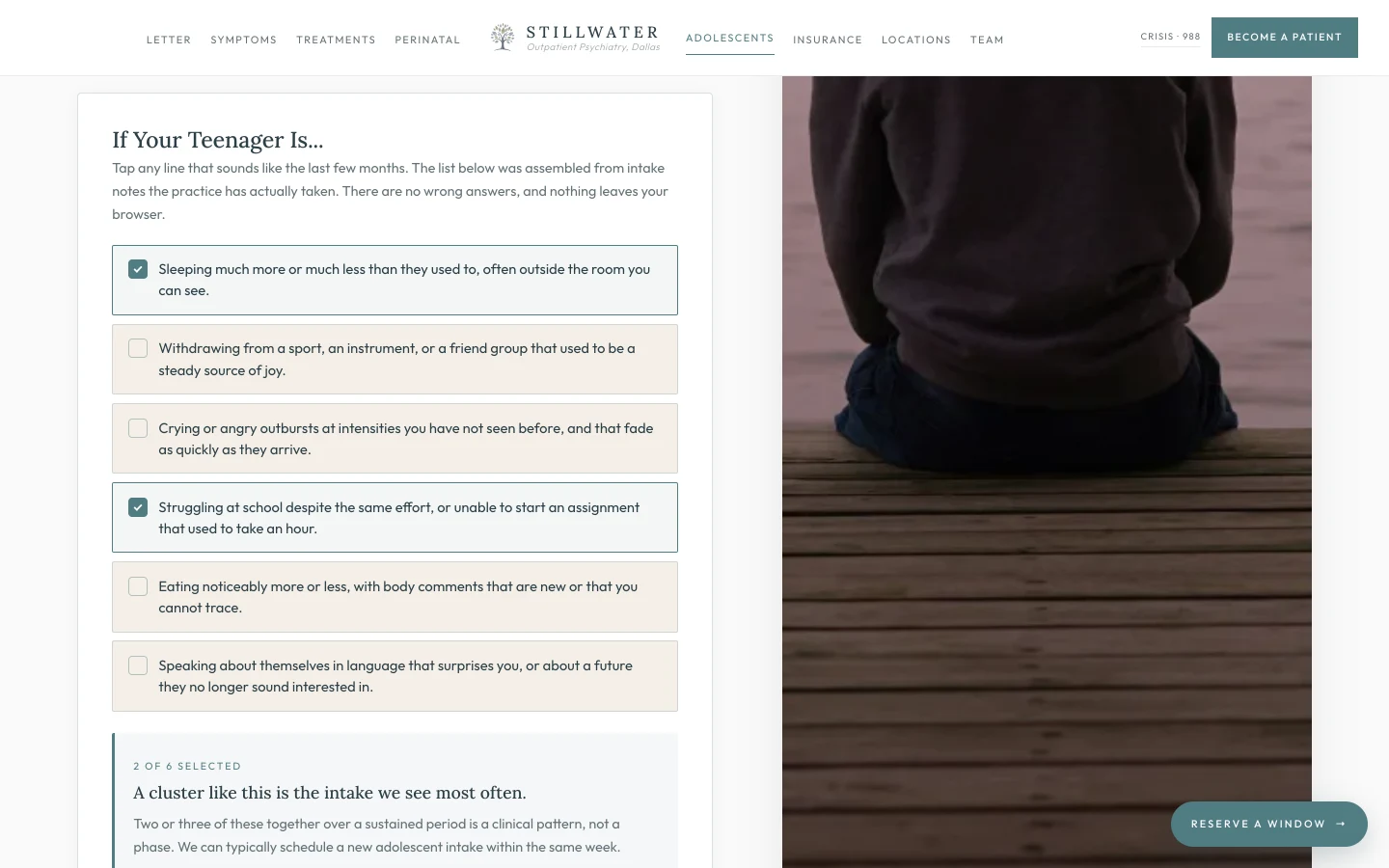
The parent of a struggling teenager is the second-hardest patient to convert in outpatient psychiatry, after the patient herself. The parent has watched the change for six or eight weeks. She has read three articles. She has thought "phase" and she has thought "depression" and she has thought "is this my fault." She has typed something into a search bar at midnight that her child does not know she typed. The brief proposes a checklist that meets her in that exact moment, in language that names the patterns she has seen, and that gives her permission to say "yes, that one" instead of forcing her to translate her observations into clinical vocabulary.
The six lines are taken directly from intake notes. Sleeping outside the room you can see. Withdrawing from a sport that used to be a steady source of joy. The wording is on purpose. A parent reads "withdrawing from a sport that used to be a steady source of joy" and recognizes the trumpet that has not come out of the case for three months. The clinical vocabulary the practice uses internally would not produce that recognition. The practice's intake vocabulary, surfaced as a tap-tap-tap interaction, does.
The summary message is tiered to the count. Selecting one returns "one pattern is enough to ask the question," with a sixty-to-ninety-minute first visit offer. Selecting two or three returns "a cluster like this is the intake we see most often," with a same-week scheduling offer. Selecting four or five returns "this is exactly what we treat," with both phone numbers in the body and an instruction to mention the pre-visit checklist at intake. Selecting all six returns "please reach out this week," with the same instruction plus the 988 line for the moment the parent realizes her child's safety is the question. Each tier is the right answer for the parent who has selected that tier. None of the tiers are sales copy. All of the tiers are how the practice would actually triage a parent's call.
What Each Insurance Plan Actually Costs Here
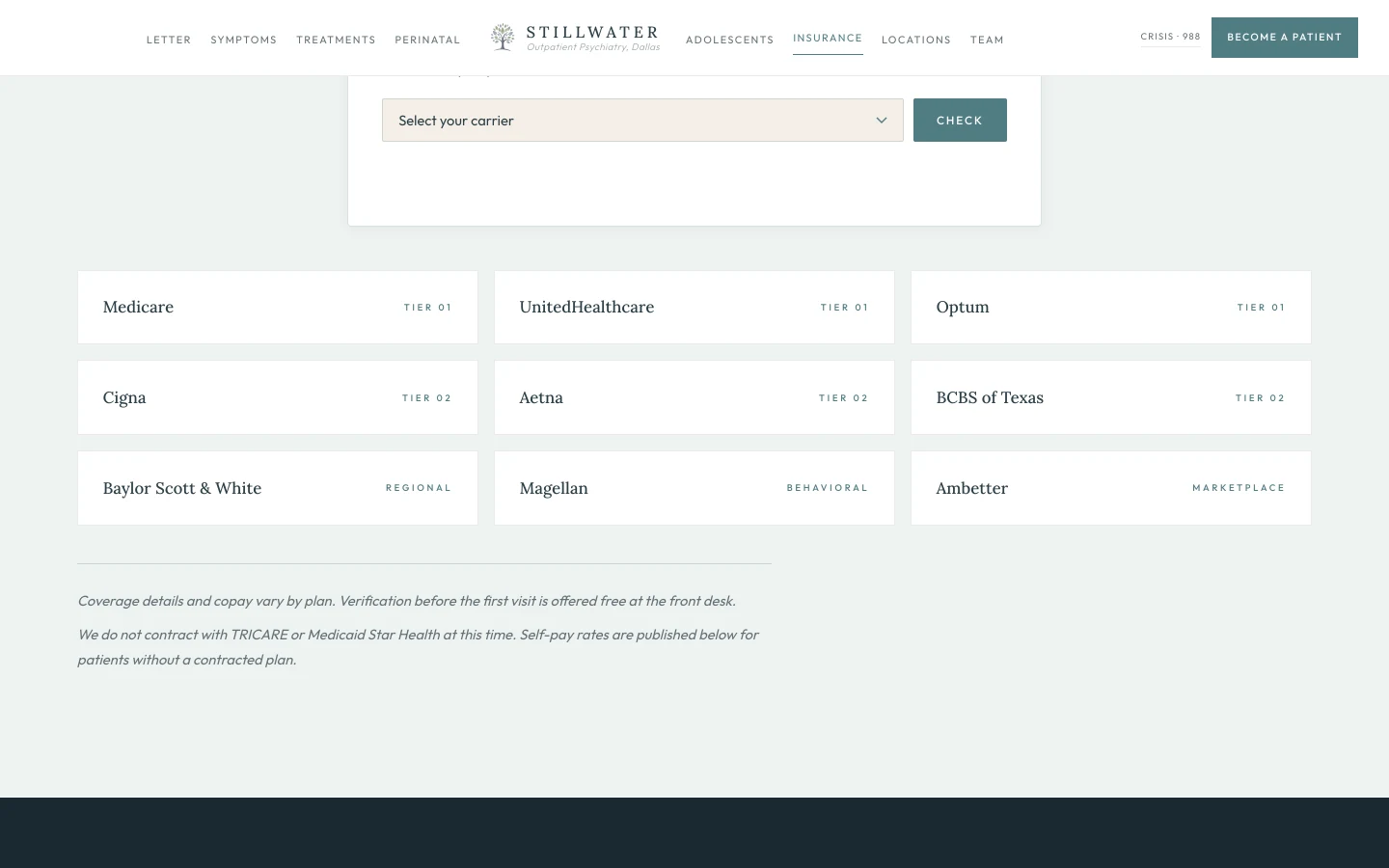
The insurance surface is the second-highest-converting surface on a psychiatry site, behind only the booking page itself. A patient in a depressive episode is calculating, on the same evening she is calculating whether to call, exactly what the visit will cost her. A practice that publishes its contracted carriers in the same typography as the headline removes the friction of the third phone call and shortens the path to the first appointment by days.
The brief proposes promoting the carrier list from a sidebar item to a full destination surface, ordered for visual scan, with the two structural admissions that earn the patient's trust. The first is the short italic line under the grid that names the carriers the practice does not contract with, by name, so a TRICARE patient learns the answer on the page rather than in a denied claim. The second is the second italic line, "Self-pay rates are published below," which signals that the practice has the same architectural commitment to self-pay patients that it has to in-network patients. Most practices publish neither. A practice that publishes both is signaling that the negotiation is not the asymmetry it pretends to be.
The carrier ordering itself is deliberate. Medicare in the first slot is the practice's geriatric patient anchor and a credibility signal to any referring primary-care physician working with a Medicare population. UnitedHealthcare and Optum are the two-card combination the patient inside that network recognizes immediately. Cigna, Aetna, and BCBS of Texas render in the second tier, the four large national carriers a typical employer plan flows through. Baylor Scott & White is the regional credential that closes the loop with the patient already inside the BSW network for primary care. Magellan is the behavioral-health-specific carrier a patient with employer-sponsored mental-health coverage recognizes by name. Ambetter is the marketplace plan many low-deductible patients in the region carry. Nine carriers, alphabetized at first glance, ordered for revenue and credibility on second glance, transparent on every glance.
Coverage Explained Without the Jargon
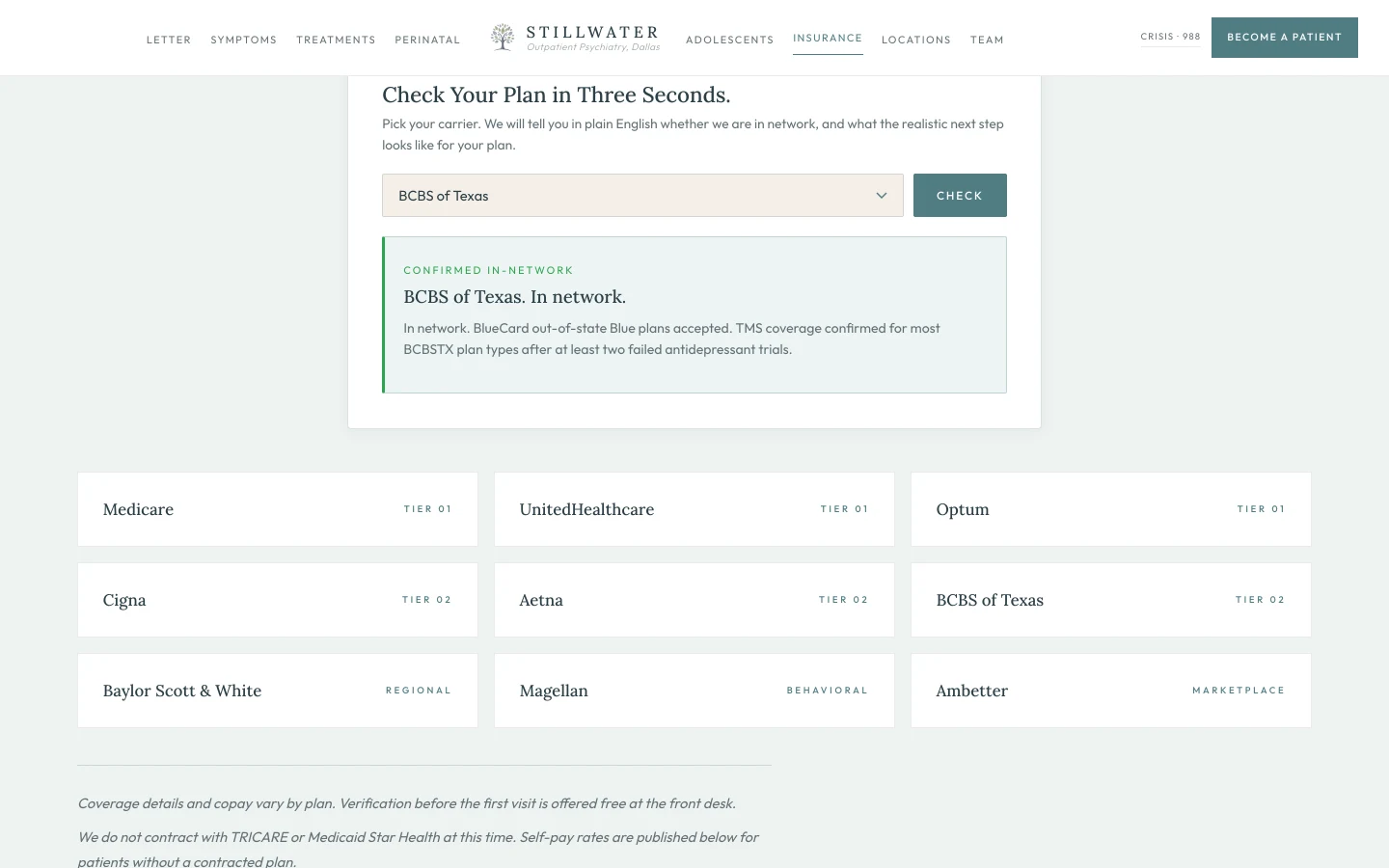
The published-carrier grid above this surface is the structural commitment to honesty. This surface is the operational commitment to speed. A patient who has called three psychiatry offices and been told "we accept most major insurance, please call back during business hours for verification" has been trained by the category to expect a phone call before she can plan. The brief proposes shortening that loop to three seconds.
The carrier dropdown carries every plan the practice contracts with, plus the four explicitly out-of-network plans the patient is most likely to ask about. Selecting a contracted plan returns a green-bordered confirmation panel with the carrier name, a coverage line specific to that carrier, and the realistic next step. BCBS of Texas confirms BlueCard acceptance and names the TMS prior-auth precondition. Aetna confirms TMS for major depression and Spravato for adults with TRD, both with prior auth that the practice files. Magellan names the underwriting plan as the variable that determines copay, and points to the verification call. Each panel is the answer the practice would give the patient on the phone, rendered in writing, with the realistic constraint named rather than papered over.
Selecting an out-of-network plan returns an amber-bordered panel with the same operational honesty. TRICARE returns "we do not currently contract with TRICARE, out-of-network reimbursement may apply, we can provide a CMS-1500 superbill for self-submission, and our self-pay rate is published on the financials sheet." Self-pay returns the actual rates: $425 initial evaluation, $185 follow-up, sliding scale availability limited and confirmed at intake. The amber panel is not a rejection. It is the operational map that lets the patient who is out of network plan around it.
The 720 millisecond verifying spinner between selection and result is the editorial pacing. A real-time response reads as a stunt. A 720-millisecond pause reads as the practice taking the question seriously. The same UX cadence the practice's intake desk would use on the phone, transposed to the patient's browser.
One Chart Across Two Texas Locations
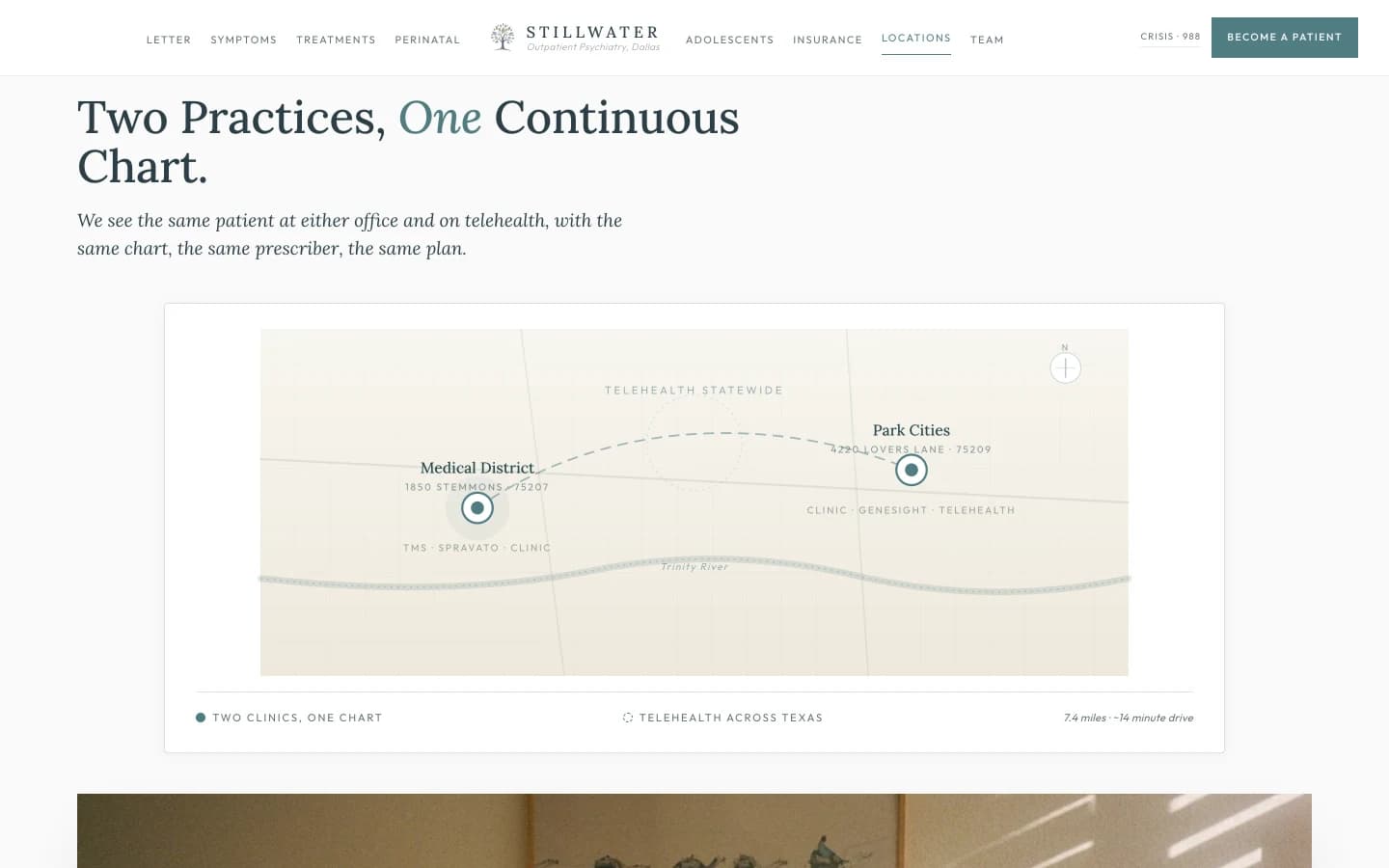
The two-location surface is where most multi-site psychiatry practices accidentally telegraph the worst thing a patient can hear. Two offices, two different staffs, two different intake forms, no record continuity, the patient explains her medication history twice. The brief proposes the opposite architecture, rendered in a single sentence the patient can carry in her head. "We see the same patient at either office and on telehealth, with the same chart, the same prescriber, the same plan."
The Medical District card and the Park Cities card are deliberately different in shape because the offices are different in shape. Medical District is the hospital-adjacent flagship, where the TMS device is housed, where the Spravato sessions are administered under the FDA REMS protocol, and where the hospital-system referral relationships sit. The Park Cities card is the suburban office, sized for medication management and intake, accessible to the patient in Highland Park, University Park, and Lakewood who would rather not drive to Stemmons for a thirty-minute follow-up. Each card names the building, names what is delivered on site, and names where the patient parks. That last detail, the parking line, is the operational courtesy most medical websites omit and most patients notice the moment they pull into an unfamiliar lot at 8:45 in the morning.
The telehealth band beneath both cards closes the architecture. "Virtual visits are available statewide for patients in Texas, including comprehensive evaluations, medication management, and ongoing care." The supporting line is the structural commitment. "The same prescriber. The same chart." A patient who started at the Medical District office, who moved to telehealth during a January ice storm, who came back to Park Cities for a follow-up, sees one prescriber and one chart through the entire arc. That continuity is the invisible product the practice is selling, and the brief renders it visible.
Shared Providers Across Both Practices
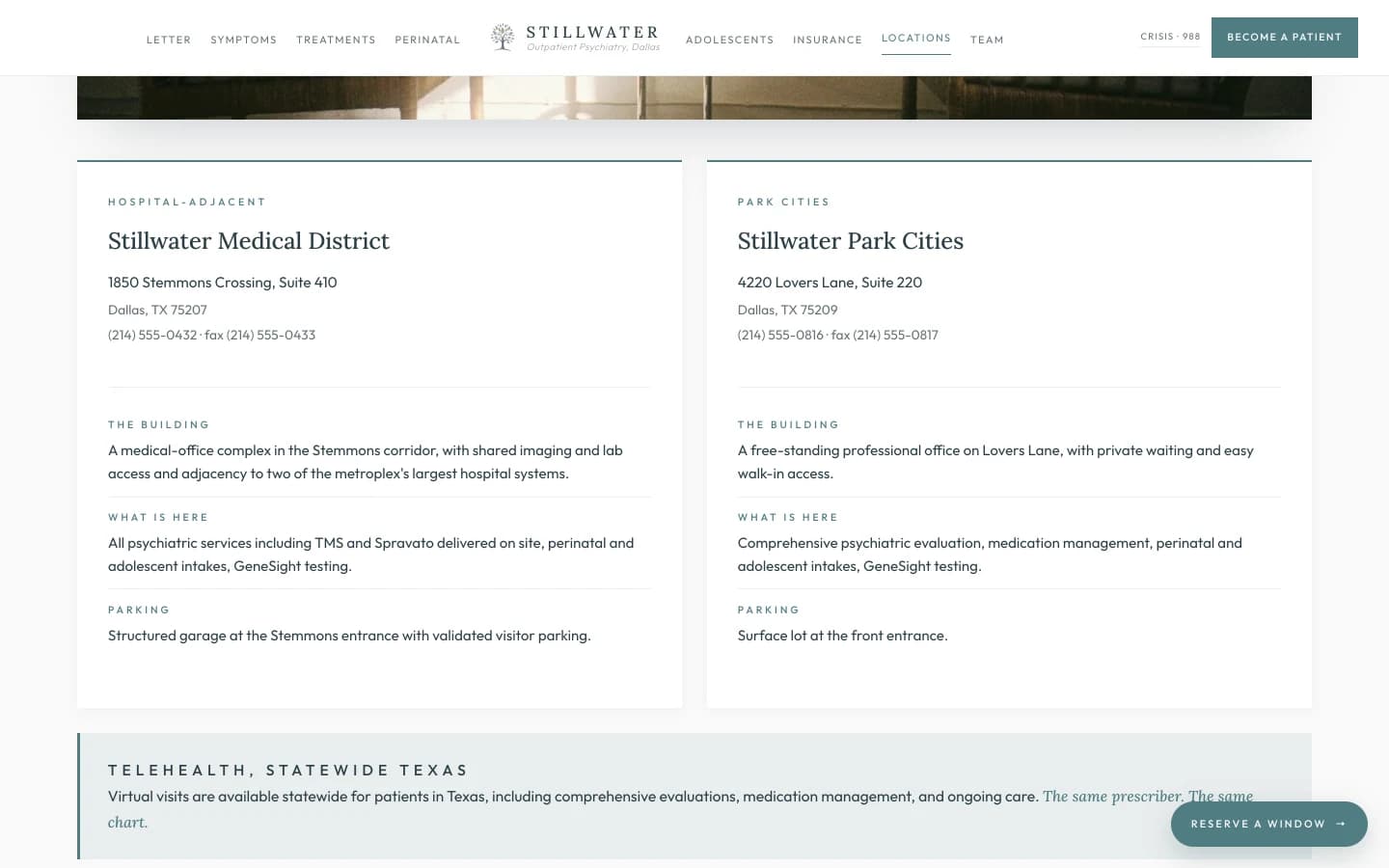
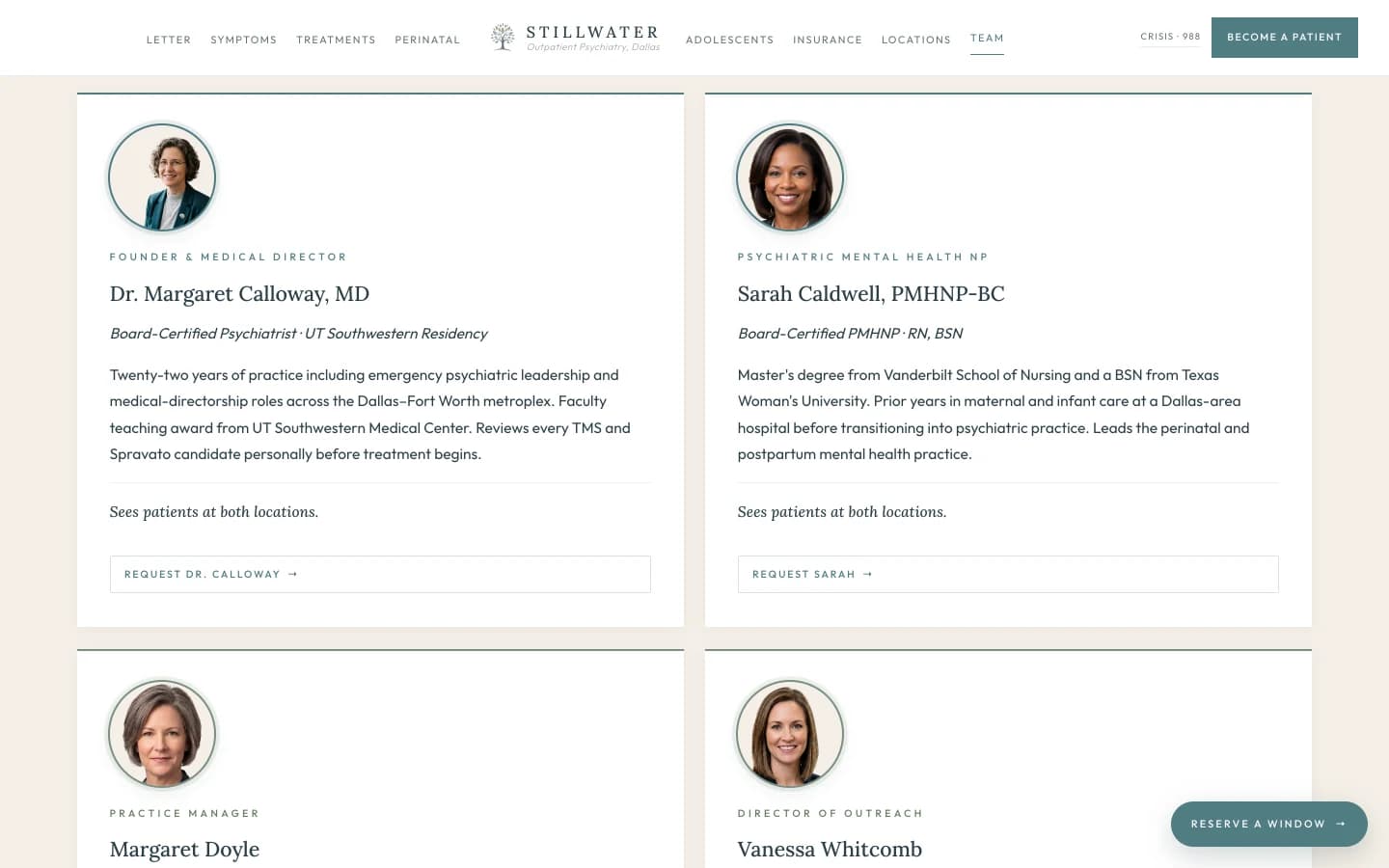
The animated map above this surface names the geography. This surface names the buildings. The two-chair photograph at the top is the architectural argument that the patient is sitting in the same room at either address, because the chairs are the same chairs in the same orientation, lit the same way, and the printed intake form on the side table is the printed intake form the practice has handed every new patient at every location for the duration of the practice's existence.
The two cards beneath the photograph are the operational continuation of the architectural argument. The address, the phone, the fax. The Building line that contextualizes the office: a medical-office complex in the Stemmons corridor with shared imaging and lab access at Medical District, and a free-standing professional office on Lovers Lane at Park Cities. The What Is Here line that names the on-site treatments at each address. The Parking line that pre-empts the question every new patient asks the front desk on the day of the first visit.
This surface is the operational rebuttal to the failure mode the brief is fighting against. Most multi-location psychiatry practices in Dallas treat the second location as a satellite, with a different prescriber, a different chart, and a different waiting experience. The brief proposes the opposite. The same patient, the same chart, the same prescriber, the same chair. The cards are how that promise is rendered in writing. The chairs are how that promise is rendered in light.
The People You Will Actually See
The team surface is the structural commitment that distinguishes a real medical practice from a brand. Most psychiatry sites publish four or five smiling headshots with serif names and a generic credential ("Provider," "Clinician," "Mental Health Specialist") that does not disambiguate who is licensed to prescribe and who is not. The brief renders the practice's actual structure, with the line between clinical providers and operational staff drawn explicitly on the page.
The two clinical cards do the conversion work. The Founder card carries the residency, the teaching award, the leadership history, and the operational commitment that earns the TRD surface above. "Reviews every TMS and Spravato candidate personally before treatment begins." A patient who is considering Spravato wants to know, before she walks in, that the medical director is reviewing her chart, not delegating the review. The PMHNP card carries the dual credential that earns the perinatal surface above. Maternal and infant care experience first, then psychiatric care, then board-certified PMHNP. That trajectory is the credential, named in three lines.
The two operational cards are the structural honesty that earns the rest of the page. Most practices either omit their operational staff entirely, or smuggle them onto the team grid with a vague "Administrative Lead" credential that lets a patient assume they are seeing a clinician. The brief proposes naming both operational roles explicitly and labeling them, in writing, "Not a clinical provider." That two-word commitment is the line that distinguishes a practice that respects the patient's question of who-is-treating-me from one that obscures it. The operational team's real years of experience are real credentials for the operational roles they hold. The brief honors them by naming the roles correctly, which is the same act of respect the brief asks the practice to extend to its patients.
What the First Visit Sounds Like
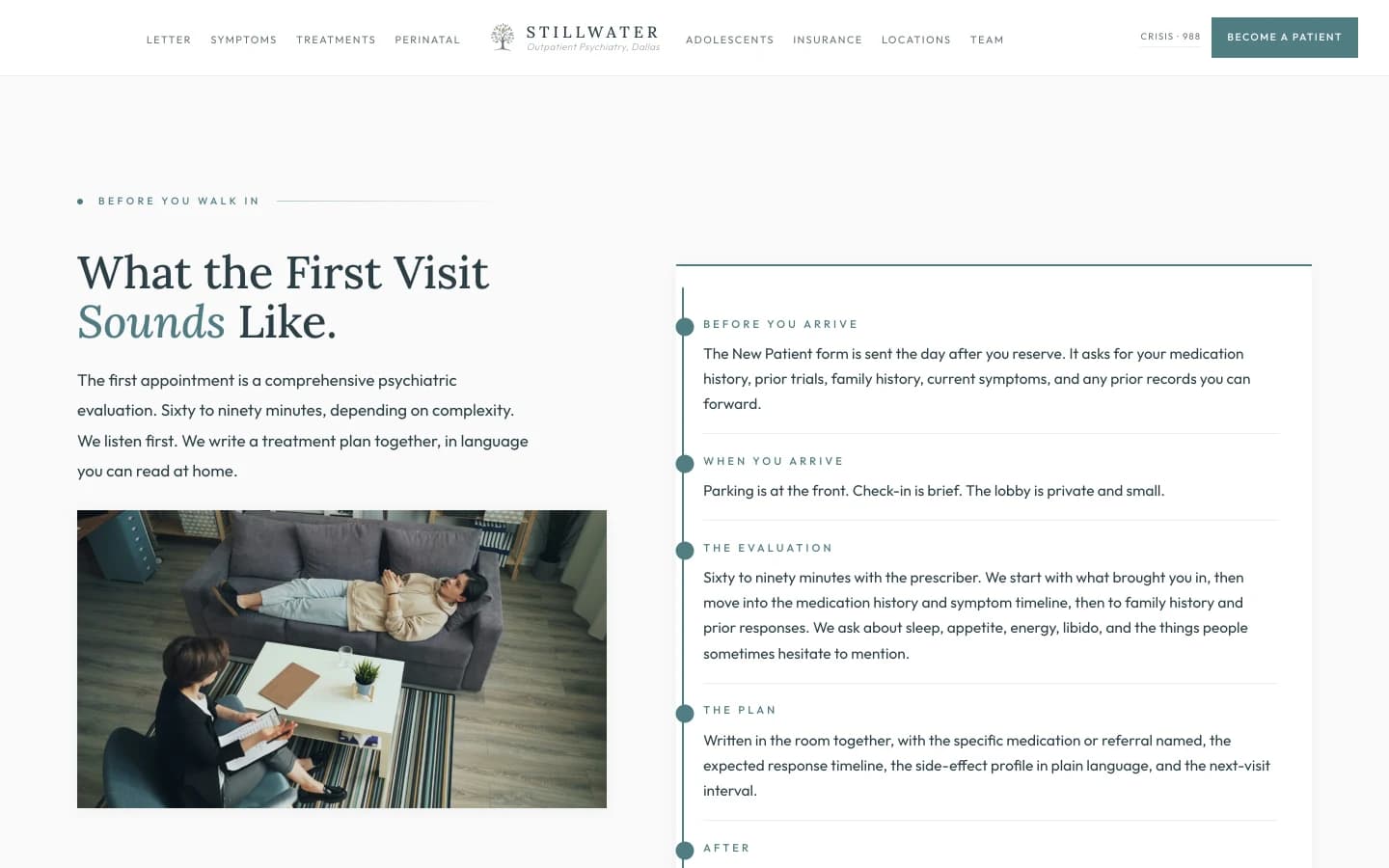
The first-visit surface is the conversion surface for the patient who has been avoiding the appointment for months because she does not know what is going to happen inside the room. Most psychiatry sites resolve this question with a single line, "Your first visit will include a comprehensive psychiatric evaluation," and leave the rest to the patient's imagination. That sentence is technically correct and operationally useless. A patient who has avoided psychiatric care for a year and has finally decided to call needs to know what she is walking into, in the same level of detail she would expect from a dentist's first visit page.
The five-row architecture in the right column is the answer. BEFORE YOU ARRIVE names the New Patient form and the records-forwarding step. WHEN YOU ARRIVE names the parking and the lobby. THE EVALUATION names the duration, the conversational arc, and the topics the patient will be asked about, including the topics most patients hesitate to volunteer. THE PLAN names the deliverable: a written treatment plan, a named medication or referral, an expected response timeline, a side-effect profile in plain language, and a next-visit interval. AFTER names the prescription send, the follow-up booking, and the care-coordination line.
The single most important sentence on the surface is the one in THE EVALUATION row. "We ask about sleep, appetite, energy, libido, and the things people sometimes hesitate to mention." That sentence does the structural work of telling the patient she is allowed to mention them, and that she will not be the first patient who does. A first-visit surface that names libido, alcohol, intrusive thoughts, and the rest of the topics that the standard "comprehensive psychiatric evaluation" line glosses over is a surface that earns the patient's full disclosure on the day of the visit, which is the difference between an effective initial regimen and a mistargeted one.
When You Should Not Wait
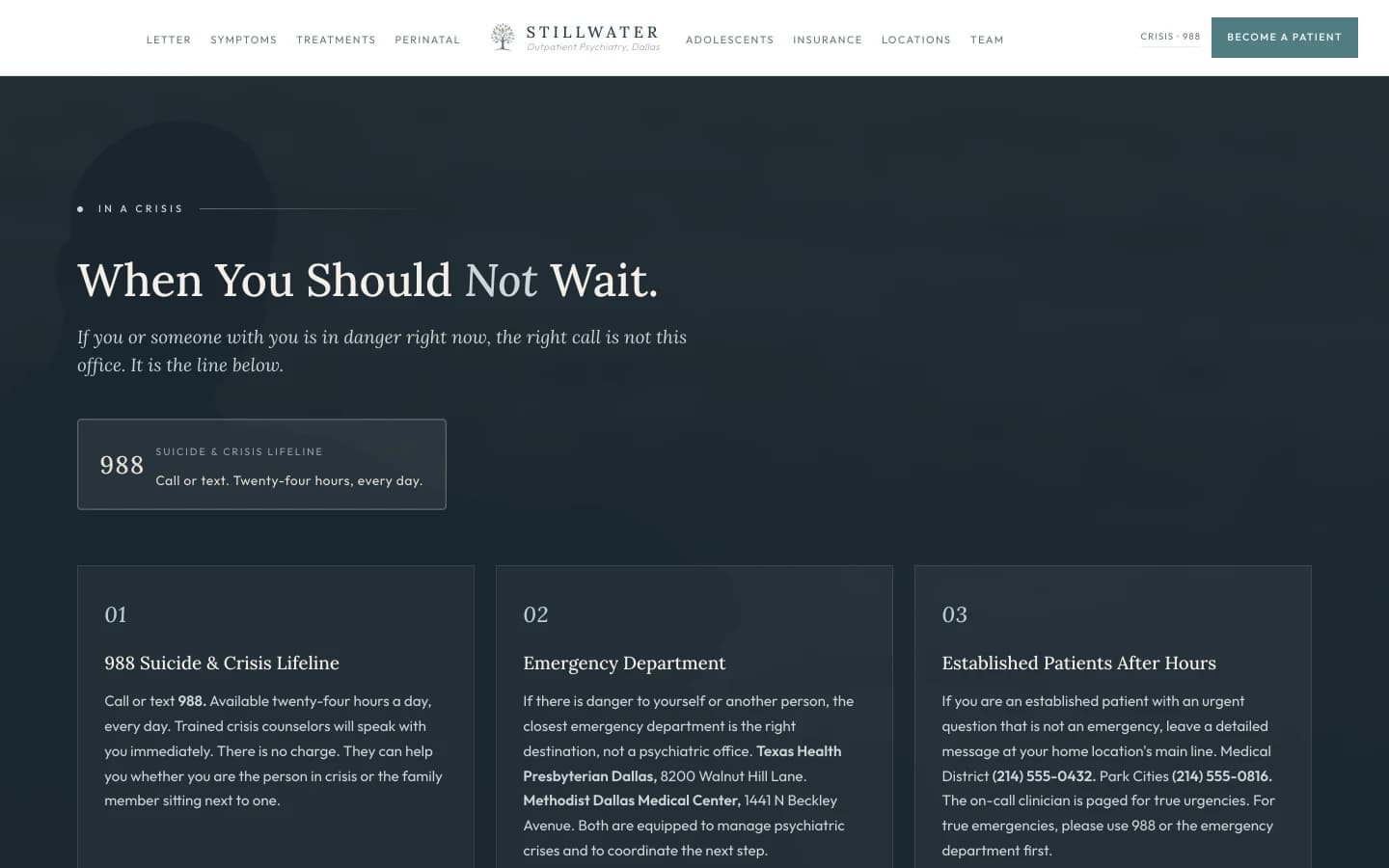
This is the surface most outpatient psychiatry sites omit, and it is the surface a metroplex psychiatry practice has the highest moral and operational obligation to render. A patient in active crisis arriving on the practice's home page at 11pm on a Sunday should not have to navigate to a contact form to learn that the right next call is 988 and the right next destination is the closest hospital ED. The brief proposes putting that information on its own surface, in a deep slate field that signals gravity in the page hierarchy, with the practice's own after-hours number named at the bottom for established patients with non-emergency urgent questions.
The three cards are deliberately ordered to match the patient's actual decision tree. Card one, 988, is the right call for almost every crisis situation, including the family member sitting next to the patient. The card explains that 988 is free, twenty-four-hour, and trained for both the person in crisis and the support person. Card two, the emergency department, names two real Dallas hospitals by name and address. Texas Health Presbyterian Dallas. Methodist Dallas Medical Center. Both are real emergency departments with the capacity to manage a psychiatric crisis. Card three is the established-patient after-hours surface, which routes urgent-but-not-emergency questions through the practice's own line with a clear ladder back to 988 and the ED for true emergencies.
The italic closing line is the architectural humility that earns the surface. "Outpatient psychiatry is the right setting for most of the work. The settings above are the right setting when the work cannot wait." That sentence does the work most psychiatry sites refuse to do, which is to tell the patient, in writing, that there are situations in which calling this office is the wrong call. A practice that is willing to say that out loud is a practice that has earned the right to be called when calling it is the right call.
Where REMS, NPI, and the Good Faith Estimate Live
![Footer section: a deep slate field that anchors the bottom of the page. The left column carries the wordmark Stillwater Psychiatric in cream serif, an italic line reading "Outpatient Psychiatry of Dallas," a short paragraph noting the practice is physician-led with all clinical decisions reviewed by a board-certified psychiatrist and treatments performed on site by named clinicians, and a small sage underline reading "Website by DBJ Technologies." A second column under Medical District lists 1850 Stemmons Crossing, Suite 410, Dallas, TX 75207, the phone (214) 555-0432, and the fax (214) 555-0433. Beneath, a Reach Us block carries three underlined links: Call the Front Desk, Become a Patient, Patient Portal. A third column under Park Cities lists 4220 Lovers Lane, Suite 220, Dallas, TX 75209, the phone (214) 555-0816, and the fax (214) 555-0817. Beneath, an Hours block lists Monday through Friday operating hours and a Closed Saturday and Sunday note. A fourth column under Find Us lists Google, Healthgrades, and Psychology Today, plus a single underline labeled Telehealth, Statewide Texas. A bottom block in small sage caps reads Licensure and Compliance, followed by a single calm paragraph: Founder and Medical Director Margaret Calloway, MD, Texas Medical Board License [number on file], NPI [number on file], DEA [registration on file]. Psychiatric Mental Health Nurse Practitioner Sarah Caldwell, PMHNP-BC, Texas Board of Nursing License [number on file], NPI [number on file]. Stillwater Psychiatric is a physician-owned medical practice operated under Texas Medical Board oversight, complies with the Health Insurance Portability and Accountability Act, patient health information held in confidence and shared only with written authorization, Notice of Privacy Practices and treatment-specific consents provided in writing at every initial visit. Spravato is administered on site under the FDA Risk Evaluation and Mitigation Strategy program. A final quiet line, set apart from the practice's own voice, reads "Template demonstration by DBJ Technologies. Not an operating practice. All names, license placeholders, phone numbers, and addresses are illustrative." A bottom strip carries the copyright "© 2026 Stillwater Psychiatric. All rights reserved." plus links to Privacy, Notice of Privacy Practices, Good Faith Estimate, and Accessibility.](/design-briefs/psychiatry-practice/12-footer.webp)
The footer is the regulator's surface and the patient's last reassurance. A psychiatry footer that does not list a Texas Medical Board license number, a Board of Nursing license number for the PMHNP, NPIs for both clinicians, a DEA registration for the prescriber, a HIPAA compliance line, and a Spravato REMS attestation is a footer that has not earned the medical word in its name. The brief proposes publishing all of them.
The Licensure and Compliance block is the surface most psychiatry sites refuse to spend the pixels on. The two clinicians named, with state-board license numbers, with NPIs, with the DEA registration that disambiguates a prescribing psychiatrist from a non-prescribing therapist, with the HIPAA paragraph that names the Notice of Privacy Practices and the consent-in-writing protocol. The Spravato line is the regulatory commitment specific to a TRD-capable practice. Spravato is administered under an FDA-mandated Risk Evaluation and Mitigation Strategy program that requires on-site supervision, two-hour observation, and documentation. A footer that names the REMS program by acronym is signaling to a referring primary-care physician, a credentialing committee, or a patient with a healthcare background that the practice has read the regulatory framework and is operating inside it.
The four navigation columns above carry the operational footing. Medical District and Park Cities as named columns with addresses and phone numbers and faxes, Hours as a calendar including the closed days, Find Us naming Google and Healthgrades and Psychology Today as the three reputation surfaces a psychiatry patient actually checks. The Telehealth, Statewide Texas link is the fourth doorway for the patient who lives outside the metroplex. The "Website by DBJ Technologies" credit sits quietly in the brand color, framed as a closing seal rather than a brag. The Good Faith Estimate link in the bottom strip is the No Surprises Act compliance most healthcare footers in 2026 still omit. This is what an outpatient psychiatry footer looks like when it is built by someone who has read the Texas Medical Board advertising rule, the HIPAA Privacy Notice requirements, the Spravato REMS protocol, the No Surprises Act, and the WCAG accessibility statement in full.
Build It For Real
Want this architecture, executed for your practice?
I build the version of this that ships. Designed end to end, launched on production grade infrastructure, with the surfaces above tuned to your actual book of business.